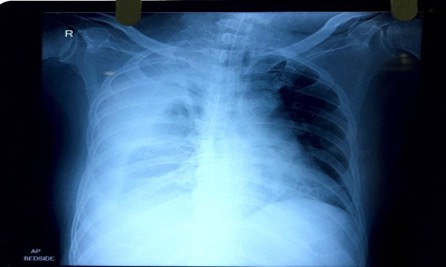
A 73-year-old male patient came with complaints of right upper and lower limb weakness, sudden onset of breathlessness and chest pain on breathing for the last few days. He is a known case of hypertension and diabetes. He was admitted for further evaluation and management. MRI showed chronic infarcts with gliosis in left parietal and temporal lobes. X-ray chest showed a large right sided pleural effusion. An intercostal drain of size 28 was inserted at 5th intercostal space in mid axillary line to drain the pleural fluid which was sent for analysis.
The pleural fluid was completely drained. The analysis showed it to be exudative in nature with lymphocytic pleocytosis on the basis of which it is presumed to be tubercular in etiology. During hospital stay patient was treated with anti-tubercular therapy coupled with other supportive measures. After Intercostal drainage, patient’s condition gradually improved. Neurology and psychiatry consultation was done, and treatment was given accordingly. Patient was discharged in hemodynamically stable condition.